
Researching breast reduction surgery can feel overwhelming, especially when you start exploring different incision methods. The technique your surgeon uses affects how much tissue can be removed, how long recovery takes, and how visible your scars will be.
This article breaks down anchor vs lollipop vs donut breast reduction techniques side by side. You’ll walk away knowing exactly which questions to ask at your consultation, and what separates these approaches at a clinical level.
Anchor vs Lollipop vs Donut Breast Reduction: Quick Comparison
| Anchor (Wise Pattern) | Lollipop (Vertical) | Donut (Periareolar) | |
| Scar Shape | Circle + vertical + horizontal line along breast fold | Circle + vertical line down to breast fold | Circle around the areola |
| Number of Incisions | 3 | 2 | 1 |
| Tissue Removal Capacity | 500g–1,000g+ per breast | ~300–500g per breast | Up to ~150–200g per breast |
| Ideal Starting Cup Size | DD–G+ | D–DDD | B–D |
| Return to Light Work | ~1 week | ~1 week | ~1 week |
| Full Recovery | 2–4 weeks | 2–4 weeks | 2–4 weeks |
| Complication Tendency | Low to moderate | Low to moderate | Lowest (least invasive) |
| Surgeon Preference | Most widely performed | Often recommended in younger patients with good skin elasticity | Uncommon for reduction, mostly used in breast lift surgery with or without implant placement |
Which Breast Reduction Technique Is Right for You?
No single technique is best for everyone. Your anatomy drives the decision more than personal preference does.
The anchor is a good fit if you need a large reduction of four or more cup sizes, have significant sagging, or carry a lot of extra skin that needs to be removed along with the tissue.
The lollipop is a good fit if you want a moderate two-to-four cup size reduction, have reasonably good skin elasticity, and want to minimize scarring without limiting results.
The donut is a good fit if you’re looking for a small one-to-two cup size reduction with minimal sagging, and your priority is the shortest possible scar.
What Each Incision Looks Like
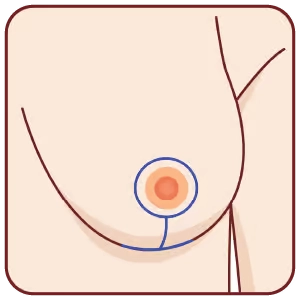
The anchor (or Wise pattern / inverted-T) technique adds a third incision. It keeps the two lollipop incisions and adds a horizontal cut along the natural breast fold. The combined scar resembles an anchor or upside-down T. This gives the surgeon the most access for reshaping and tissue removal.
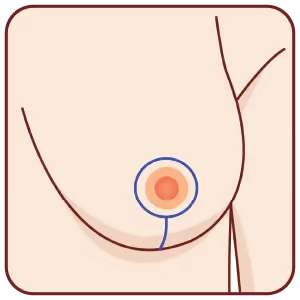
The lollipop (or vertical) technique uses two incisions. One circles the areola, and a second runs straight down from the bottom of the areola to the breast fold. Think of the shape of a lollipop: the circle is the candy, the line is the stick. This technique removes tissue primarily from the lower and outer breast.
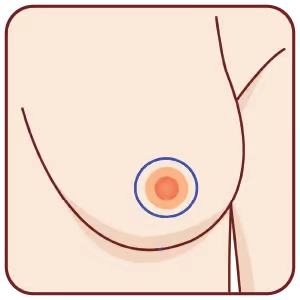
The donut (or periareolar) technique uses a single circular incision. It goes around the edge of the areola, right where the darker skin meets the lighter skin. The scar stays hidden at that natural border, making it the least visible of the three.
Recovery Time by Technique
All three techniques are performed as outpatient procedures, and patients typically go home the same day. Early recovery milestones are similar across the board, but the anchor technique often involves removing a greater amount of breast tissue, which can push full recovery out slightly.
For all three techniques, most patients can expect:
- Around 1 week before returning to desk work or light activity
- 2–4 weeks for full recovery
- Up to 12 months for scars to fully fade and soften
The donut technique typically has the smoothest early recovery, as there’s less disruption to the breast tissue overall. The lollipop technique avoids the horizontal incision, which can reduce the amount of initial swelling compared to the anchor approach. The anchor technique involves the most extensive tissue work. Some patients find they need the full 4 weeks before feeling comfortable with all daily activities.
Scar care starts after the first few weeks. Silicone sheets, gentle massage, and consistent sun protection all help scars fade faster. Most scars become thin, pale lines by the 12-month mark.
Nipple Sensation: What the Research Shows
Preserving nipple sensation is a top priority in breast reduction surgery. The results depend more on the pedicle (how the surgeon keeps the blood and nerve supply to the nipple intact) than on the incision pattern alone.
The pedicle is essentially the tissue bridge that stays connected to the nipple during surgery. It carries the blood vessels and nerves that keep the nipple viable and responsive to sensation. Surgeons choose different pedicle types depending on how much tissue needs to be removed and which incision pattern they’re using.
The most common options are:
- Inferior pedicle: The nipple stays attached to a bridge of tissue at the lower part of the breast. This is the most widely trained technique and is most often paired with the anchor incision. It’s highly reliable but involves a longer tissue bridge in larger reductions, which can put more strain on the nerve supply.
- Superomedial pedicle: The nipple stays attached to tissue from the upper inner portion of the breast. It’s most often paired with the lollipop incision. The shorter pedicle length is thought to better protect the nerves, and it has strong sensation data to back that up.
- Superior pedicle: Similar to the superomedial, but the tissue bridge comes from directly above the nipple. Used less frequently today.
- Free nipple graft: Used only in very large reductions where the nipple must travel too far to stay attached. The nipple is fully detached and reattached as a graft. Sensation is largely lost with this approach.
Knowing which pedicle your surgeon plans to use matters as much as (or more than) the incision type when it comes to sensation outcomes.
A 2025 study followed 434 patients undergoing breast reduction with the superomedial pedicle technique. The study found that 78.1% of breasts maintained or improved nipple sensation after surgery, with younger age and lower BMI associated with better sensation outcomes.
For comparison, the free nipple graft technique, which is sometimes used in very large reductions, showed sensation preservation in only 22.2% of cases in the same study. A separate analysis found that the medial pedicle preserved normal-to-near-normal sensation in approximately 85% of patients, while the superior pedicle came in closer to 67%.
Surgeon Preference: Who Uses Which Technique?
Recent research indicates that a majority of breast reductions are performed using the inferior pedicle, most commonly paired with the anchor (Wise pattern) incision. Only 25% used the superior or superomedial pedicle, which is most often paired with the vertical (lollipop) approach.
However, experienced surgeons usually don’t have a “preferred” method, as it depends on the patient’s anatomy, goals, and the amount of breast tissue that’s being removed. It’s essential to choose a surgeon who can explain which technique they intend to use for your procedure (and why), and can show you before and after results from their previous patients.
When choosing a surgeon, ask these questions directly:
- Which technique do you recommend for my anatomy, and why?
- How many breast reductions have you performed?
- Are you trained in anchor vs lollipop vs donut breast reduction approaches?
Schedule a Consultation to Learn More
Every breast is different. The right technique is the one your surgeon chooses after a thorough evaluation of your anatomy, ptosis (sagging), and goals. At Harris Plastic Surgery, Dr. Stephen U. Harris, MD FACS, brings nearly 30 years of surgical experience and thousands of breast reductions to every consultation. His team also handles insurance coordination from start to finish, so there are no surprises on your bill.
To learn whether an anchor vs lollipop vs donut breast reduction is right for you, schedule a consultation today. You can also contact us by phone/text.

Stephen U. Harris, MD FACS
Dr. Stephen U. Harris is a board-certified plastic surgeon and recognized expert in breast reduction and reconstruction surgeries, having performed thousands in his career. When it comes to patient care, his philosophy is that every surgery should improve his patient’s overall quality of life, not just their appearance. Dr. Harris stays up-to-date on all the latest advancements in breast augmentation, reconstruction, and reduction and is a recognized innovator in the field. In fact, he was the first surgeon at Good Samaritan Hospital to offer primary prepectoral implant breast reconstruction, as well as secondary prepectoral revision surgery.
Dr. Harris also serves as Chief of Plastic Surgery at Good Samaritan Hospital in West Islip, New York, and is an active staff surgeon (and former Chief of Plastic Surgery) at South Shore University Hospital in Bay Shore, New York.